You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
The immediate replacement of a single missing tooth with a dental implant in the esthetic zone is among the more challenging scenarios faced by clinicians. As such, it requires special attention to planning and execution at each stage of treatment and often necessitates the modification of "standard" implant workflows. The delivery of a provisional restoration immediately following placement of an implant and graft materials is justified and advantageous when specific criteria are met.1-4 Immediate provisonalization protocols are not appropriate for every implant site; therefore, the careful consideration of key risk criteria is essential to case selection and to improve the prognosis and predictability (Table 1). For example, implants with low primary stability, such as those with insertion torque values less than 20 Ncm or implant stability quotient (ISQ) values less than 60, as well as a high occlusal or functional load, a lack of buccal bone, or the presence of active periodontal disease are all factors that increase the risk of a poor prognosis for immediate provisionalization protocols. Implants with a high primary stability of greater than 30 Ncm or an ISQ value greater than 65 decrease the risk of a poor prognosis for immediate loading protocols. Other factors that decrease the risk of a poor prognosis include low functional loads, the presence of sufficient buccal bone, and implants that are placed 3 to 4 mm below the intended cementoenamel junction (CEJ).
There are both advantages and disadvantages associated with this treatment (Table 2). Specific advantages of immediately provisionalizing implants in the esthetic zone include preservation of the existing gingival architecture, the early development of emergence contours, and the ability to better estimate the final treatment outcome. Disadvantages of provisionalizing implants at the time of placement include increased risk of implant failure and the need for patient compliance with a soft diet. When immediately placed implants are provisionalized at the time of placement, patients initially benefit by the rapid return to form (ie, esthetics) but not to function because they are not to "use" the provisional restoration. At the definitive stage, both patients and clinicians benefit from the increased esthetics and predictability that are provided by a properly designed provisional restoration.5-8
The immediate placement of an implant into an extraction socket requires surgical skill and experience. Whether placed freehand, fully statically guided, partially statically guided, or with dynamic navigation, the implant must be in the correct 3-dimensional position and demonstrate high stability. Beyond appropriate placement and stability of the implant, the provisional restoration should be designed and fabricated to support the peri-implant soft tissues while providing space for favorable maturation and migration of the gingiva.9-12 It must also be reasonably esthetic and grossly out of the path of the opposing dentition, both in the maximal intercuspal position (MIP) and in excursive contacts, to minimize the forces placed on the integrating implant and surrounding bone.13-15
Patient and Site Selection
Successful management of the esthetic zone with immediate implant provisionalization requires specific conditions regarding the patient's occlusion and oral health as well as for the recipient bed. To immediately provisionalize an implant in the esthetic zone, the patient's periodontal health should be ideal, the occlusion should be normal (eg, no deep bite), and there should be no signs of grinding/bruxism. Requirements for the recipient bed include the absence of inflammation or other pathoses, an intact alveolar socket on the labial aspect, sufficient bone width and height to permit adequate initial implant stability, and healthy gingiva.
Treatment Planning and Surgical Template Fabrication
The diagnostic workup should include the patient's medical history, medications, dental history, and expectations as well as an intraoral examination and a cone-beam computed tomography (CBCT) scan. When conducting the intraoral examination, an evaluation of the soft-tissue volume and contours should be performed. The most important soft-tissue structures to identify and measure are the interproximal papillae on either side of the edentulous site. The papillae should be symmetrical with those of the same tooth on the contralateral side. If one or both of the papillae associated with the implant site is absent or insufficient, a soft-tissue augmentation procedure should be performed before implant placement and immediate provisionalization.
If the soft-tissue volume is acceptable and the tooth to be replaced is still present, the 3-dimensional CBCT scan should show its incisal position in relation to the tooth in the opposing arch. If the patient is missing the tooth to be replaced, the radiographic guide should show the ideal crown position, and the contours of the crown should be visible on the CBCT scan that is taken. The radiographic guide may then be converted into the surgical template. The surgical template should show the labial surface of the future crown to limit the labial angulation of the implant. Ideally, screw-retained provisional crowns for anterior teeth have their access channels positioned to exit through the cingulum.
Hard- and Soft-Tissue Requirements
When considering immediate provisionalization of a single implant in the esthetic zone, one of the keys to successful treatment is ensuring that there is sufficient hard- and soft-tissue volume. Having sufficient tissue volume permits the restorative team members to fabricate a natural appearing implant-supported restoration. The volume of bone available must be sufficient in both height and width. For implant placement, the width of the alveolar ridge should be a minimum of 3 mm wider than the diameter of the selected implant. Furthermore, a minimum of 2 mm of facial bone thickness should be maintained to provide support for the gingival tissue contours.1 Regarding the gingival tissue, the quality is as important as the quantity. An appropriate gingival phenotype and width of attached gingiva are necessary to provide the contours to achieve esthetic results.
Implant and Component Selection
The body shape and abutment connection of the implant selected are extremely important when considering immediate provisionalization. To assist in achieving sufficient initial stability of the implant to permit provisionalization, the implant body shape recommended is a tapered design with aggressive, sharply pitched threads. The abutment connection should allow for ease of attachment and removal of the prosthesis using screw retention. An engaging temporary abutment is used to retain the provisional restoration.
Determining Primary Implant Stability
Gapski and colleagues identified several key factors for success in immediate implant loading protocols.2 Arguably, the most important is establishing sufficient primary stability of the implant.16 There are two methods used to determine primary implant stability. The first involves measuring the insertion torque, which is the amount of force necessary to deliver and seat the implant into the recipient bed. The advantage of this method is that most implant drivers have torque settings, so there is no need to purchase additional equipment. The disadvantages of this method include that the torque measurements on implant drivers must be calibrated on a regular basis to provide reliable readings, there is no consensus on whether regular or higher torque insertion forces are ideal,17 and the measurement can only be taken once. The second method of determining primary implant stability is to use resonance frequency analysis (RFA). RFA involves sending a magnetic wave into the implant via a transducer and then measuring the magnitude of the wave that reverberates back. The value is measured using the ISQ scale, which was developed to assist in determining loading protocols.18,19 The advantages of using this method include the ability to take sequential measurements of implant stability, which provides an easy, noninvasive method of tracking the progress of osseointegration. Patients who receive immediately provisionalized implants will have a second ISQ measurement after 6 months. The disadvantage of using this method is the need to purchase an RFA device and transducers.
Provisional Fabrication and Emergence Contours
There has been fairly extensive investigation into the best clinical parameters for immediate implant provisional restorations. Notably, Lee, Esquivel, and others have examined the concept of critical and subcritical contour areas on the emergence profiles of provisional and definitive implant abutments.9,10 Block was also hugely impactful in his early work with the concept of immediate loading.7,8
If an implant demonstrates sufficient primary stability as defined by Moy and others,16-19 clinicians have the opportunity to provide the patient with a provisional restoration at the same time or during the same day of implant placement. Patients generally appreciate the return to more normal esthetics, and the peri-implant tissues benefit from maintenance and support of the natural gingival architecture. It is far easier to maintain the delicate papillae than it is to try to reshape or recreate them once they have flattened out. In most scenarios, the papillae will flatten over the course of osseointegration and tissue maturation without the ideal support provided by a provisional restoration.
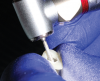
Fabrication of an immediate provisional restoration requires the selection of an appropriate implant provisional abutment and the creation of a tooth shell. Among other materials, commonly used implant provisional abutments are made from polyether ether keytone (PEEK), PEEK/titanium hybrid, or solid titanium (Figure 1). They can have engaging or non-engaging designs and are also sometimes available in various collar heights. Low-collar, engaging solid titanium provisional abutments offer advantages over others due to their high fracture strength, narrow dimensions, controllable emergence contours, ability to be torqued to high values, and robust seal at the implant abutment junction. However, they present the disadvantages of being slightly more expensive, harder to cut, and metallic in color. The metallic color can be mitigated by applying a flowable opaquing composite resin prior to attaching it to the crown shell. Solid titanium provisional abutments are best cut with a high-speed carbide bur or a metal cutting disc on a straight handpiece. They will heat up during cutting, but this can be easily managed by grasping them with a hemostat or analog and occasionally placing them into a cool water bath. The tooth shell can be fabricated from composite using a stone or resin model (Figure 2 through Figure 10) or from the patient's existing tooth or crown.
The key design parameters of the immediate provisional restoration are those of its emergence zone. This is the area between the head of the implant and the supragingival crown. The emergence contour of the provisional restoration should be as narrow as possible for the first 1 to 2 mm from the head of the implant and then gently flow into the contours of the crown at the CEJ. This narrow portion ensures that there is a maximum amount of space for biologic graft materials, blood clotting, and swelling. The gentle S-curve contour into the crown helps to support but not compress the peri-implant gingiva. When trying in the immediate provisional restoration, there should be no blanching of the gingiva. It is also advantageous to leave a moderate amount of open space in the gingival embrasures. This provides room for the soft tissues to migrate incisally during the healing and maturation stages. If the provisional restoration is designed using these parameters, the result will generally be an excess of soft tissue following osseointegration.
Clinical Protocol and Case Examples
A step-by-step clinical protocol for the immediate provisionalization of single implants is outlined in Table 3. Key factors for the delivery of immediate implant provisional restorations include a narrow emergence contour in the lower 2 mm of the provisional restoration, no blanching or compression of the peri-implant gingiva, an undercontoured facial emergence, open gingival embrasures, maximum stability and seal at the implant abutment junction, and a total lack of occlusion in MIP and throughout the excursive paths.
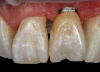
To demonstrate the principles and protocols described in this article, three case examples are included. The first case involves the treatment of a patient who sought replacement of the maxillary left canine (tooth No. 11) with an implant-supported restoration (Figure 11 through Figure 34), and in the second case, the patient presented for replacement of the maxillary left central incisor (tooth No. 9) (Figure 35 through Figure 44). In the third case, the patient also presented for replacement of the maxillary left central incisor (tooth No. 9) but had a preexisting bonded pontic made from the natural tooth. This was utilized in lieu of a composite tooth shell to fabricate the immediate provisional restoration. (Figure 45 through Figure 57).
Postoperative Guidelines
Immediate provisonalization of a dental implant will place loading forces on it, so it is important to minimize these forces, especially lateral ones, as much as possible. The most dangerous loading forces are generated by lateral or excursive movements. As was previously mentioned, when the patient's mouth is closed, occlusal contact may be controlled by reducing the incisal height of the provisional restoration. However, forces can still be applied to the implant with a bolus of food while chewing or with the tongue during speech. Patients whose implants are immediately provisionalized should be instructed to stay on a "nonchewing" diet and to be careful when speaking during the initial period of 6 to 8 weeks. This instruction minimizes the loading forces on the immediately provisionalized dental implant.
Other critical instructions to provide to these patients include how to care for the surgical site with at-home hygiene. Many patients are concerned about not damaging or harming the surgical site, and for others, the surgical site is painful to touch, so they stop performing home hygiene care. This permits plaque to build up on the sutures as well as the wound edges. With the buildup of bacteria, healing may be delayed, increasing the chances for wound dehiscence. To minimize the accumulation of plaque, patients should be instructed to start gently rinsing with warm saline on the second day. Patient should also be encouraged to use a cotton swab soaked in a mixture of mouthwash and hydrogen peroxide to "wipe" around the gingival margins to remove debris and plaque.
Conclusion
The proper design and delivery of an immediate provisional restoration when placing a single implant in the esthetic zone offers benefits regarding the patient experience, in the creation and maintenance of the peri-implant gingiva, and more. When implants are placed in ideal positions with sufficient primary stability, this procedure adds minimal risk to the implant's osseointegration while increasing the likelihood of a more ideal esthetic outcome.
Queries regarding this course may be submitted to authorqueries@broadcastmed.com
About the Authors
Todd R. Schoenbaum, DDS, MS
Professor of Restorative Sciences
Coordinator of Clinical Education in Implant Dentistry
Dental College of Georgia
Augusta University
Augusta, Georgia
Peter K. Moy, DMD
Professor of Clinical Dentistry
Nobel Biocare Endowed Chair in Surgical Implant Dentistry
Oral and Maxillofacial Surgery Section
School of Dentistry
University of California, Los Angeles
Los Angeles, California
References
1. Grunder U, Gracis S, Capelli M. Influence of the 3-D bone-to-implant relationship on esthetics. Int J Periodontics Restorative Dent. 2005;25(2):113-119.
2. Gapski R, Wang HL, Mascarenhas P, Lang NP. Critical review of immediate implant loading. Clin Oral Implants Res. 2003;14(5):515-527.
3. Cosyn J, Hooghe N, De Bruyn H. A systematic review on the frequency of advanced recession following single immediate implant treatment. J Clin Periodontol. 2012;39(6):582-589.
4. Pitman J, Seyssens L, Christiaens V, Cosyn J. Immediate implant placement with or without immediate provisionalization: a systematic review and meta-analysis. J Clin Periodontol. 2022;49(10):1012-1023.
5. Cosyn J, Eghbali A, Hermans A, et al. A 5-year prospective study on single immediate implants in the aesthetic zone. J Clin Periodontol. 2016;43(8):702-709.
6. Thanissorn C, Guo J, Jing Ying Chan D, et al. Success rates and complications associated with single immediate implants: a systematic review. Dent J (Basel). 2022;10(2):31.
7. Block M, Finger I, Castellon P, Lirettle D. Single tooth immediate provisional restoration of dental implants: technique and early results. J Oral Maxillofac Surg. 2004;62(9):1131-1138.
8. Block MS, Mercante DE, Lirette D, et al. Prospective evaluation of immediate and delayed provisional single tooth restorations. J Oral Maxillofac Surg. 2009;67(11 Suppl):89-107.
9. González-Martín O, Lee E, Weisgold A, et al. Contour management of implant restorations for optimal emergence profiles: guidelines for immediate and delayed provisional restorations. Int J Periodontics Restorative Dent. 2020;40(1):61-70.
10. Gomez-Meda R, Esquivel J, Blatz MB. The esthetic biological contour concept for implant restoration emergence profile design. J Esthet Restor Dent.2021;33(1):173-184.
11. Schoenbaum TR, Chang YY, Klokkevold PR, Snowden JS. Abutment emergence modification for immediate implant provisional restorations. J Esthet Restor Dent. 2013;25(2):103-107.
12. Schoenbaum TR. Abutment emergence profile and its effect on peri-implant tissues. Compend Contin Educ Dent. 2015;36(7):474-479.
13. Kan JYK, Rungcharassaeng K, Deflorian M, et al. Immediate implant placement and provisionalization of maxillary anterior single implants. Periodontol 2000. 2018;77(1):197-212.
14. Saito H, Chu SJ, Reynolds MA, Tarnow DP. Provisional restorations used in immediate implant placement provide a platform to promote peri-implant soft tissue healing: a pilot study. Int J Periodontics Restorative Dent. 2016;36(1):47-52.
15. Chu SJ, Salama MA, Salama H, et al. The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compend Contin Educ Dent. 2012;33(7):524-534.
16. Shiffler K, Lee D, Rowan M, et al. Effect of length, diameter, intraoral location on implant stability. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016;122(6):e193-e198.
17. Atieh MA, Baqain ZH, Tawse-Smith A, et al. The influence of insertion torque values on the failure and complication rates of dental implants: a systematic review and meta-analysis. Clin Implant Dent Relat Res. 2021;23(3):341-360.
18. Rowan M, Lee D, Pi-Anfruns J, et al. Mechanical versus biological stability of immediate and delayed implant placement using resonance frequency analysis. J Oral Maxillofac Surg. 2015;73(2):253-257.
19. Baltayan S, Pi-Anfruns J, Aghaloo T, Moy PK. The predictive value of resonance frequency analysis measurements in the surgical placement and loading of endosseous implants. J Oral Maxillofac Surg. 2016;74(6):1145-1152.